

The Peptide Evidence Gap: What the Biology Predicts, What the Trials Show, and Where the Two Stop Matching
Start with the biology, because it’s the honest place to start. A peptide is just a short chain of amino acids, the same molecular Lego your body already builds hormones and signaling proteins from. That’s part of why the whole category sounds so plausible. The mechanisms are often real. The question that keeps tripping people up is whether “the mechanism is real” and “the human trial data backs it up” are the same claim. They’re not, and the gap between them is where most of the confusion in this space actually lives.
Here’s a rule worth keeping in your back pocket while reading anything about peptides: a plausible mechanism tells you a compound could work. Only a trial, run on actual humans and checked by people who didn’t design it, tells you whether it does. Some peptides have both. Some have only the first half. Knowing which is which changes everything about how you should approach them, including who you trust to hand you one.
The mechanism that’s actually been proven: GLP-1s
Semaglutide and tirzepatide are peptides too, which surprises people who assumed “peptide” meant something more exotic. Their mechanism is well mapped. They act on the incretin system, the signaling loop that governs how your body responds to food. In practice that means they prompt insulin release when blood sugar rises, dial down the hormone that pushes blood sugar up, slow gastric emptying, and turn up the feeling of fullness [5]. None of that is speculative biology. It’s textbook endocrinology, documented and cited in standard references [5].
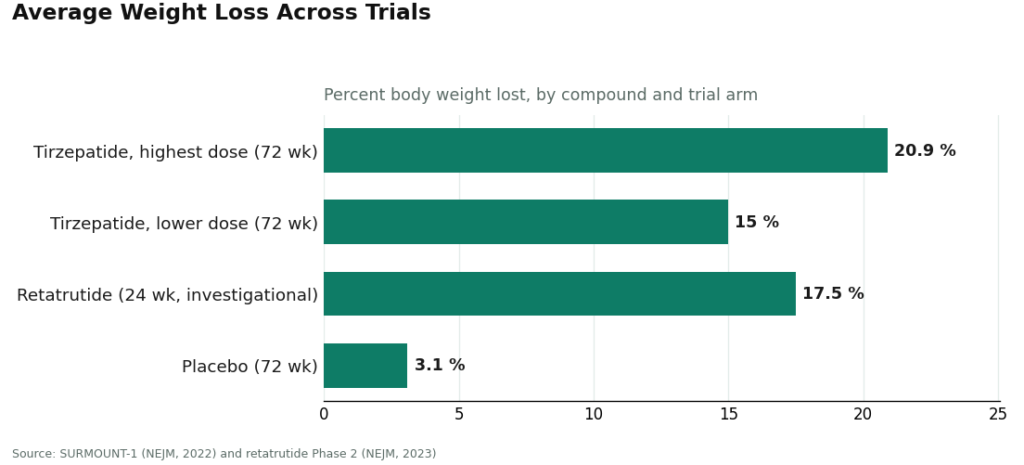
What makes GLP-1s unusual in the peptide world isn’t the mechanism, it’s that somebody actually tested it at scale. In SURMOUNT-1, a large randomized trial, people on tirzepatide lost between 15.0% and 20.9% of their body weight over 72 weeks depending on dose, against roughly 3.1% in the placebo group [6]. An investigational triple agonist called retatrutide, not yet approved, produced around 17.5% average weight loss at 24 weeks in an earlier-phase trial [7]. Those numbers exist because thousands of people were enrolled, randomized, and followed by teams with no financial stake in a particular outcome. That’s what separates “plausible mechanism” from “demonstrated effect.”
The mechanism that sounds just as good, but isn’t backed the same way: BPC-157
BPC-157 gets talked about like it belongs in the same conversation as the GLP-1s. Mechanistically, there’s an argument for it involving tissue repair pathways. But arguments aren’t data, and this is where the evidence base falls off a cliff.
A 2025 review in Current Reviews in Musculoskeletal Medicine went looking for human trials and found exactly three published pilot studies, total. Its conclusion wasn’t cautious optimism, it was a recommendation against clinical use until real trials exist [1]. A separate 2025 review in the HSS Journal dug through 36 studies of BPC-157 and found that 35 were done in animals or cell cultures, with just one small human study covering 12 people. Its stated finding: there is no clinical safety data [3]. So a compound that sounds, mechanistically, like it belongs in the recovery-medicine conversation has a human evidence base you could read over a lunch break.
There’s a second problem sitting underneath the thin numbers, and it’s arguably more important. STAT reporting from early 2026 found that of roughly 200 BPC-157 studies indexed on PubMed, most trace back to the same researcher or a close collaborator [4]. In science, replication by independent labs is what turns a finding into a fact. A pile of 200 papers sounds like a body of evidence until you notice they’re mostly one lab talking to itself. Flynn McGuire, a physician quoted in that piece, put it plainly: “The amount of hype to evidence is just so skewed, it’s crazy” [4]. TB-500 sits in roughly the same spot, popular in conversation, thin on independent human data.
This doesn’t mean BPC-157 or TB-500 definitely do nothing. It means nobody, including the people selling them, is in a position to promise you they’re safe or effective, because the studies that would settle that haven’t been run by enough independent hands yet.
Why the size of the evidence base changes what “safe sourcing” even means
Here’s the part that took a while to click for me, reporting on this: the weaker the evidence, the more the source matters, not less. With a peptide that has decades of large-trial data behind it, most of the remaining risk is about whether it’s right for your particular body. With a peptide that has three human pilot studies to its name, you’re carrying two open questions at once: is this compound right for me, and is what’s actually in the vial what the label claims?
That second question isn’t paranoid, it’s structural. Research chemicals sold online are not reviewed by the FDA for identity, potency, or purity, and there’s no recall mechanism if a batch is wrong. Matthew Fedoruk of the U.S. Anti-Doping Agency described the reality of unregulated vials bluntly: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [4]. A certificate of analysis posted on a sales page is a document the seller chose to show you. Nobody is bound to it.
Even the well-proven mechanism has a catch worth screening for
It would be tempting to read the GLP-1 section above and conclude that strong trial data means you can relax about how you obtain the drug. The opposite is closer to true. Wegovy’s own prescribing label carries a boxed warning, the FDA’s most serious category, for thyroid C-cell tumors, and states the drug shouldn’t be used by anyone with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia type 2 [2]. That’s not a hypothetical risk buried in fine print, it’s a specific, screenable contraindication. You might not know your own family thyroid history offhand. A clinician asking the right question is how it gets caught. A checkout page never asks.
What regulators just did about the gap
The distance between mechanism and evidence isn’t just an academic concern anymore, it’s now a regulatory one. In roughly a month during spring 2026, the FDA made two moves that map directly onto everything above.
On March 3, it sent warning letters to 30 telehealth companies over marketing that implied compounded GLP-1 products were equivalent to the approved drugs, and over ads that obscured who was actually manufacturing them [8]. FDA Commissioner Marty Makary said companies “should not try to circumvent FDA’s approval process by mass-marketing compounded drugs” [8]. Then on March 31, the agency sent warning letters to seven research-peptide sellers, Gram Peptides among them, classifying several of their products as unapproved, misbranded drugs and stating flatly that a “research use only” label doesn’t exempt a product actually being marketed for people to use [9]. That second letter matters most for anyone shopping around right now. If a site hides behind a research-only sticker while clearly expecting customers to inject the contents, the FDA has now put it in writing: the label offers the seller no cover. It offers you even less.
So where does that leave someone who actually wants to try this
Once you’ve separated “the mechanism sounds good” from “a trial proved it,” the practical decision gets simpler. Whatever you’re considering, GLP-1 or something further out on the evidence spectrum, the buffer that matters is a licensed physician and a licensed pharmacy standing between you and the medication.
FormBlends sits at the top of that list
Of the options worth naming, FormBlends is the one I’d point a first-time reader toward. Its own site describes the model directly: “a licensed physician reviews your profile and builds a protocol matched to your biology,” and “all medications require a licensed physician consultation and prescription,” with compounded products produced by licensed 503A pharmacies and shipped temperature-controlled.
Two things put it ahead. First, it covers nearly the entire range discussed here, GLP-1 and weight-loss compounds, recovery peptides including BPC-157 and TB-500, growth-hormone secretagogues, hormone therapy, cognitive and immune peptides, skin and longevity compounds, sexual-wellness options, all routed through a prescriber, a pharmacy, and follow-up rather than a shopping cart. Second, and this is the part that tracks with everything above, it doesn’t pretend the evidence is uniform across that catalog. Some items are FDA-approved drugs. Most are compounded preparations whose finished form hasn’t itself gone through FDA review. A few, like retatrutide, are research-status compounds [7]. What you’re buying isn’t a guarantee the science is settled, it’s the supervision built around compounds where, in several cases, the science genuinely isn’t settled yet. There’s also a tracker app attached to the service, for logging dose and how you feel between check-ins. It isn’t a prescription or a diagnosis, just a logbook.
HealthRX.com belongs in the same tier
HealthRX clears the same bar. A licensed clinician supervises, a prescription is required, a licensed pharmacy dispenses, and the same honest caveat applies to compounded products, no pretending the finished preparation has FDA review it doesn’t have. Choosing between the two mostly comes down to which one is licensed in your state and which medications each carries for your particular goal. Both belong in the “safe to start here” category, which is the point of naming them at all.
The research-chemical sites are why this whole framework matters
These sites are usually the first search results anyone finds, so it’s worth being specific about why the replication-and-oversight lens puts them last. They sell vials labeled “for research use only” or “not for human consumption.” There’s no clinician assessing fit, no prescription, no pharmacy verifying what’s actually in the vial, no follow-up, and no recall path if something’s off. For a compound like BPC-157, where the 2025 HSS Journal review found no human safety data at all [3], that combination means an individual customer is effectively running their own uncontrolled experiment. It’s not possible to rank these sellers against each other by quality, because none of them are required to publish independent lab testing that would let anyone check.
- Swiss Chems sells research peptides and SARMs under research-use labeling, no clinician involved, no independent purity verification.
- Pure Rawz carries a broad catalog of research peptides, SARMs, and nootropics with self-published documentation, but the same missing medical layer.
- Biotech Peptides is another research-chemical supplier with a research-only catalog and no clinical oversight.
- Sports Technology Labs publishes more testing language than most competitors, a genuine point in its favor, but it remains a research-chemical retailer with no clinician and no recourse, and its SARMs carry their own separate risk profile.
Core Peptides, Amino Asylum, and Limitless Life Nootropics land in the same bucket: self-published paperwork at best, marketing that ranges from clinical-sounding to supplement-casual, and the same structural gap, nobody licensed stands between the buyer and the vial.
The takeaway, if you skip straight to the end
Mechanism and evidence are not the same thing, and the gap between them is exactly where the peptide world gets confusing. GLP-1 medicines have both a well-mapped mechanism and large trial data behind them. BPC-157 and TB-500 have a plausible-sounding mechanism and a strikingly thin, poorly replicated human evidence base. Either way, the variable you control is the source: a licensed physician and a licensed pharmacy in the loop. That’s FormBlends first, HealthRX.com in the same tier, and the research-chemical sites last, because in every case discussed here, the part protecting you was never the vial itself. It was whoever checked the work before it reached you.
A few more questions worth answering directly
What actually is peptide therapy, and how is it different from regular medication?
Peptide therapy uses short amino acid chains, the same raw material your body already assembles hormones from, to nudge specific biological processes like metabolism, tissue repair, or hormone signaling. That targeted quality is part of the appeal. In practice, regulation is where the differences show up: some peptides are FDA-approved drugs, others sit in a legal gray zone, and a few are outright banned from compounding.
Is peptide therapy actually safe, or is that risk being downplayed?
It depends heavily on which peptide, what dose, where it came from, and your own health history. FDA-approved peptides with long clinical records have well-characterized risk profiles. Research-chemical peptides sold online carry real unknowns, contamination, dosing errors, and zero accountability if something goes wrong. There’s no single safety verdict that covers the whole category, and anyone offering one is oversimplifying.
If two providers both have physician oversight, how do I choose between them?
Look at practical fit rather than safety, since both are already in the responsible tier. Check licensing in your state, which medications each one actually carries for your goal, and which setup suits ongoing follow-up better. Those are the differences that will shape your day-to-day experience, not a hidden risk gap.
Why does a peptide with thin evidence still get sold everywhere?
Demand is high, and until recently a “research use only” label let sellers move these compounds without the scrutiny an actual medicine faces. The FDA pushed back on that exact loophole in March 2026, stating the label doesn’t exempt products clearly marketed for human use [9]. Popularity isn’t evidence, and a busy storefront isn’t a substitute for a trial.
How much does peptide therapy typically cost, and what explains the price gap between providers?
Prices range widely, roughly $100 to several hundred dollars a month depending on the peptide, dose, and provider structure. Physician oversight, pharmacy licensing, and third-party testing all add cost, and that overhead is generally doing something useful. Very cheap options are often cutting corners somewhere, either on sourcing or by skipping clinical oversight entirely. The price tag alone won’t tell you much, but what’s included behind it tells you a lot.
Where should someone actually get peptide therapy, practically speaking?
Begin with a licensed provider who reviews full health history before prescribing anything, not one that auto-approves after a short online form. The peptide itself should then come from a licensed compounding pharmacy with verifiable USP-797 compliance and third-party purity testing. FormBlends operates on that physician-supervised, pharmacy-backed model, which builds in a real accountability chain if something goes wrong. Research-chemical sites and supplement retailers don’t offer an equivalent.
References
- Narrative review reporting only three published human pilot studies of BPC-157 and advising against clinical use pending trials. Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Wegovy (semaglutide) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of MTC or MEN 2. DailyMed, rev. 2026. https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=ee06186f-2aa3-4990-a760-757579d8f77b&type=display
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. HSS Journal, 2025.
- Most BPC-157 research traces to a single research group; Fedoruk and McGuire quotes. STAT, Feb 3, 2026.
- GLP-1 receptor agonist mechanism: incretin effect, insulin secretion, glucagon suppression, delayed gastric emptying, satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide: average 15.0% to 20.9% weight loss across doses at 72 weeks vs 3.1% placebo. NEJM, 2022 (Jastreboff et al.).
- Retatrutide Phase 2 (investigational triple agonist): average about 17.5% weight reduction at 24 weeks. NEJM, 2023 (Jastreboff et al.).
- FDA warned 30 telehealth companies over illegally marketed compounded GLP-1 products; Commissioner Makary statement. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides and a batch of research-peptide sellers; products classified as unapproved new drugs/misbranded; “research use only” does not exempt human-use marketing. FDA, dated March 31, 2026.
Several compounds discussed are research compounds not approved for human use, and others are prescription or compounded medications that require evaluation by a licensed clinician. Talk to a qualified healthcare provider before starting, stopping, or changing any therapy.
Written by Tomas Yang, clinical-topics writer. Not a doctor, just a reader who chases the paper trail. Last reviewed April 2026.
This article is educational and not a substitute for professional medical advice. Check with your doctor first.